josh farkas 💊
pulm/crit attending at U. Vermont 🐄 zentensivist 🧘♂️ FOAMite 🌊 diuresis jedi 💦 ECG nerd 🤓 resuscitationist 💉 no COI 💰
- approach to temperature of 38.1 :
- when someone gets vanco: probability #1 = they actually have an invasive MRSA infection probability # 2 = vanco levels are adequate probability # 3 = vanco doesn’t cause AKI what is (prob 1)(prob 2)(prob 3) ?

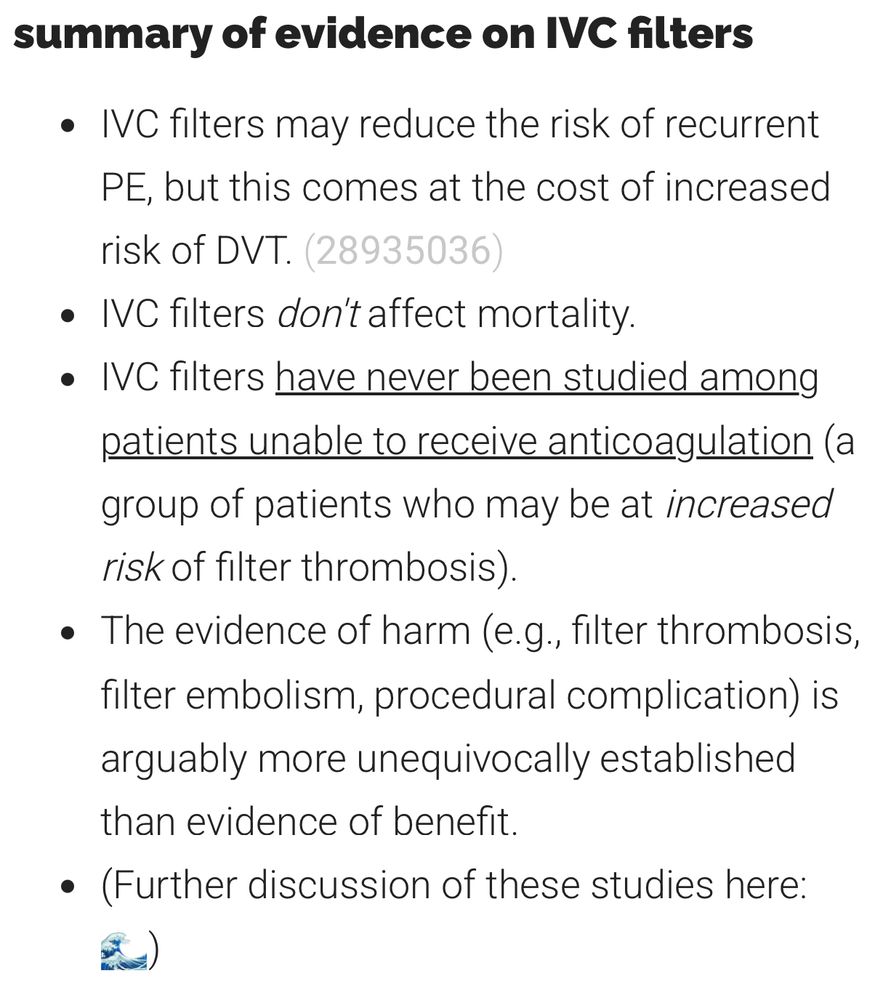
- IVC filters are not evidence-based or regulated adequately. the thread below is eye-opening but even aside from that thread, it has long been evident that IVC filters are a glorified anxiolytic rather tha legit EBM emcrit.org/ibcc/pe/#IVC_filter… #EMIMCC
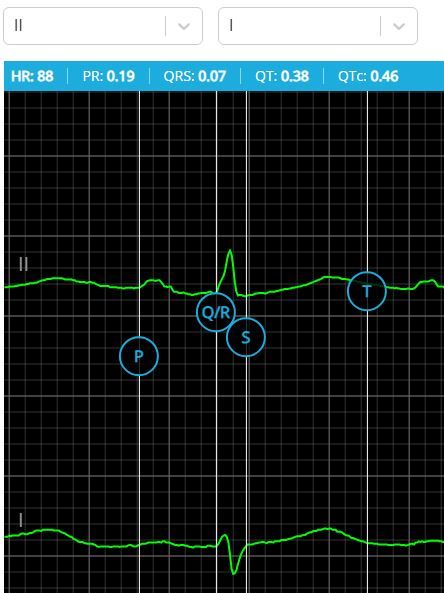
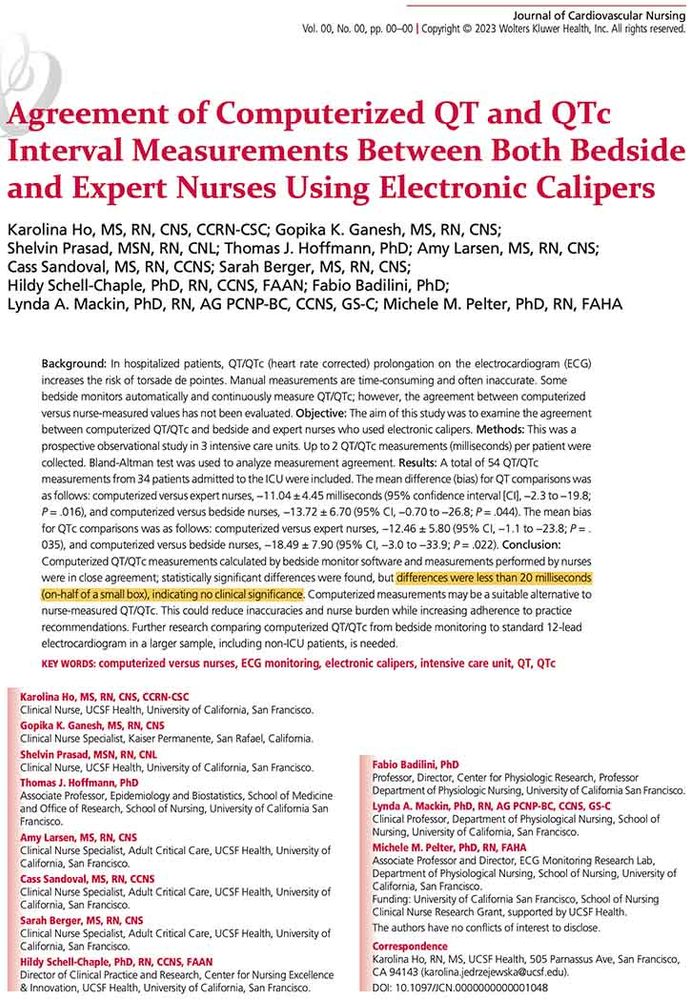
- any opinions about using electronic calipers to measure QTc from online telemetry? this is now built into our EMR so easily done from any computer w/o the delay & cost of a full ECG if the tracing is crisp, this seems fine for everyday stuff (eg hand-wringing about IV haloperidol) #EMIMCC #ECGsky
- 90% of *adult* epiglottitis patients don’t need intubation. when in doubt, give a big wack of steroid, some antibiotics, and watch like a hawk. call ICU and we can admit for obs whatever you do, please don’t rush in and try rapid sequence intubation… #1/2 #EMIMCC emcrit.org/ibcc/epiglot...

- why not RSI? if they’re truly so obstructed that they need an airway (uncommon) the safest approach is generally a double setup with awake intubation if their airway is open enough that RSI is safe, then they don’t need intubation at all either way, RSI is generally illogical #2/2

- [Not loaded yet]
- he misspelled “grifts”
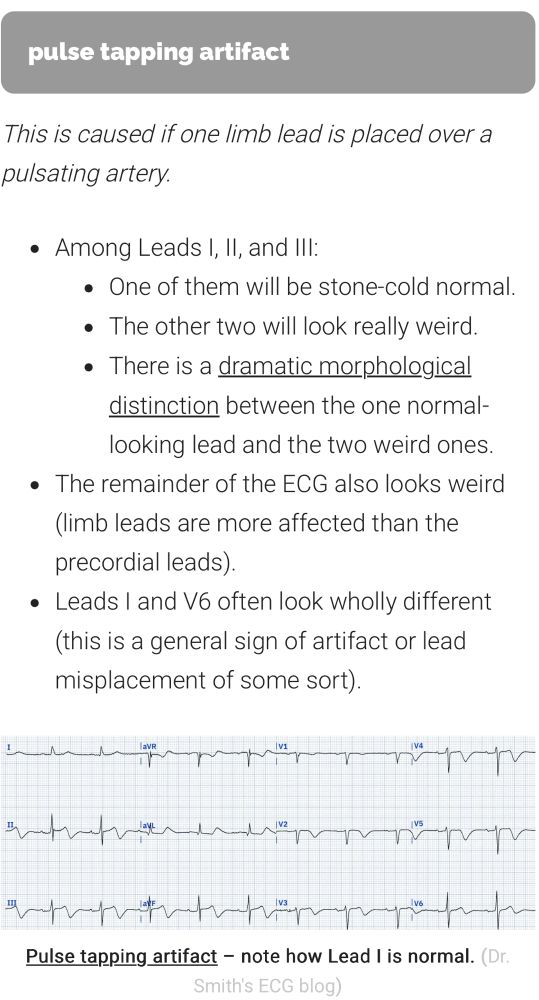
- this is a super interesting case. I don’t want to spoil it for you, so take a minute and go thru it. In the wisdom of 20/20 hindsight, can you figure out what happened?? #EMIMCC 🧵 #1/2
- I think the weird ECG was caused by pulse tapping artifact one of the limb leads is over an artery ➡️ this generates a bizzare artifact in the baseline the key clue to artifact (rather than MI) is lead III which shows a sinusoidal waviness of the baseline (not discrete STE after the QRS) #2/2
- did you think that labetalol is a single drug? nope it’s actually a mixture of FOUR different drugs RS, RR, SS, and SR-labetalol and this is clinically relevant! lets discuss why… 🧵 #1/3 #EMIMCC
- [Not loaded yet]
- Sometimes it works, sometimes it doesnt Nicardipine seems more reliable
- REMAP CAP was too underpowered to show anything or add substantially to the existing evidence base. the reason it’s getting so much press is recency bias. we have a natural tendency to get jazzed up about the newest, hottest trial while ignoring the previous dozens of trials… #1/2 #EMIMCC
- This reflects a deficit in how we are trained to read the scientific literature. We always focus on how to interpret a single study. Every journal club everywhere = 1 article. We rarely discuss how to integrate multiple divergent articles (which can actually be a lot harder).
- when given IV, bioavailability of each of these four drugs is 100% the resulting 1:1:1:1 combo has 7x more beta-blocking activity than alpha-blocking activity so IV labetalol is mostly a beta-blocker it’s an alpha/beta-blocker wannabe (this is why IV labetalol isn’t great for severe HTN) #2/3

- when given PO, the four-drug combo is subject to extensive first-pass hepatic metabolism. the liver selectively chews up *more* of the beta-blocking enantiomers the resulting combo has only 3x more beta-blocking activity than alpha-blocking activity, so PO labetalol = legit alpha/beta-bl #3/3

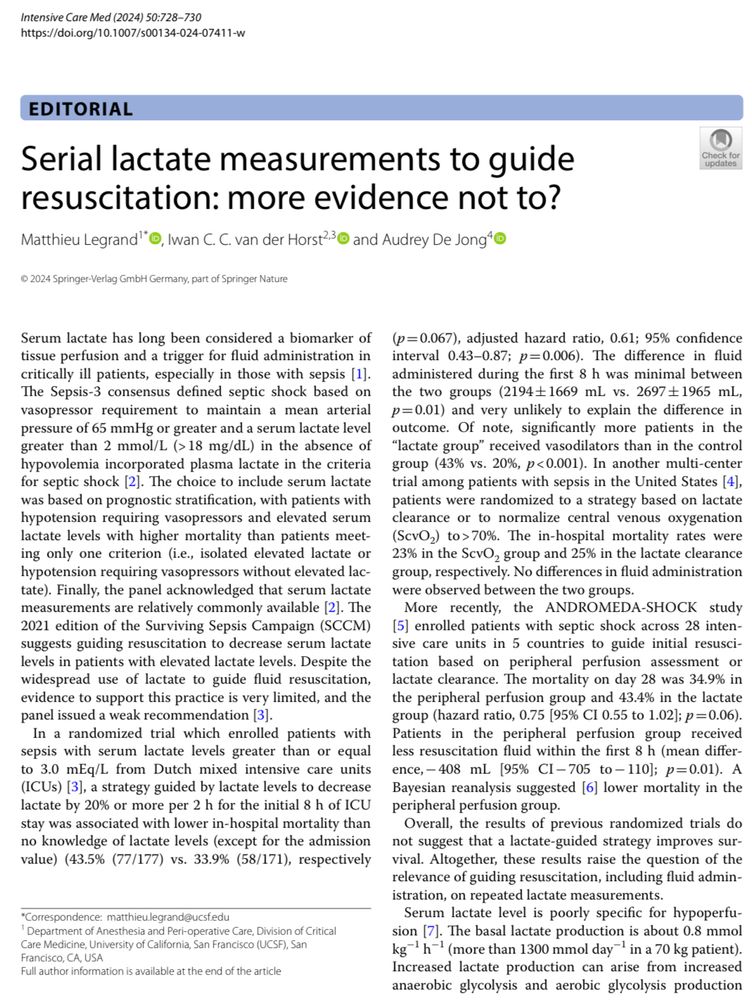
- New editorial in ICM about the dysutility of lactate as a perfusion goal in sepsis I reviewed lactate physiology & why it’s not a perfusion index 10 years ago here: emcrit.org/pulmcrit/understand… Talk more in 2035. Nothing will change #EMIMCC
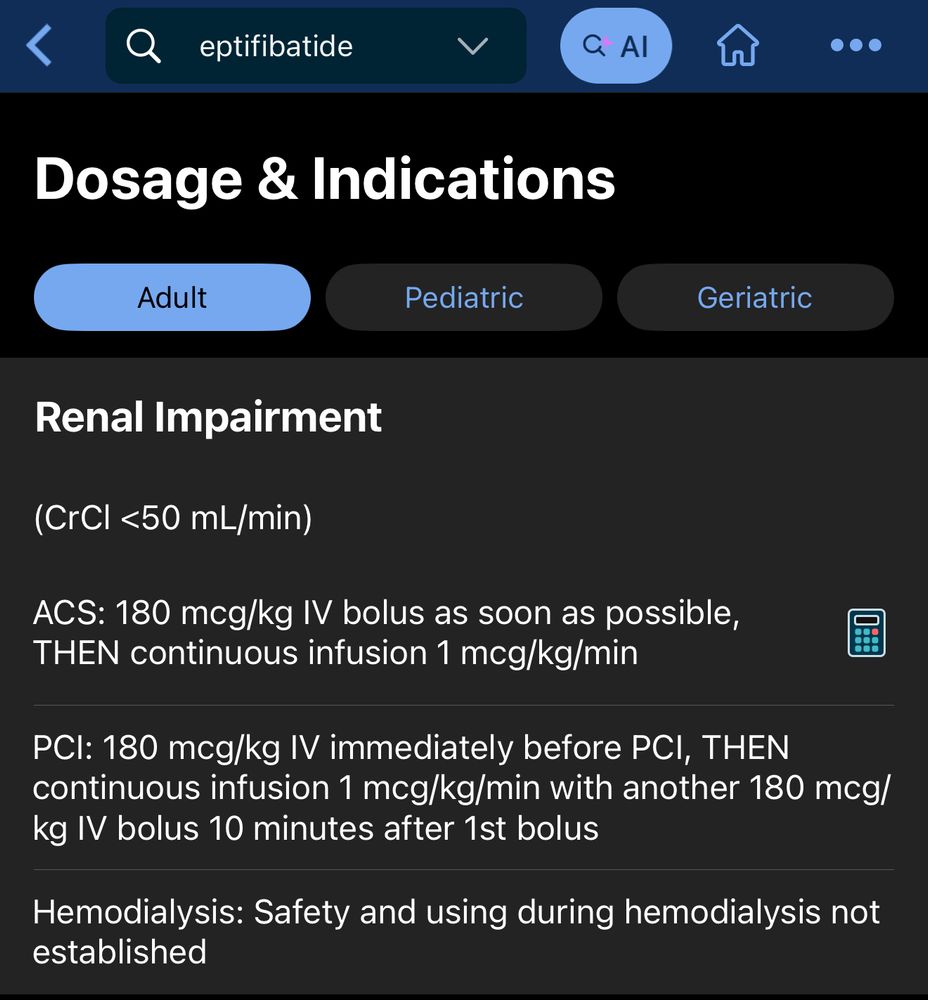
- I want to talk about a patient who died when I was a trainee. He presented with an MI & was treated w/ the usual therapies along with an eptifibatide infusion (an antiplatelet gtt which was commonly used back then). He developed agitated delirium refractory to numerous medications… #EMIMCC #1/5

-
View full threadAnd to this day, the published dosing of eptifibatide doesn’t make much sense. You’re supposed to dose-reduce for GFR <50. But it doesn’t really make sense to give the same dose for GFR 49 & GFR 10 (the drug is renally cleared) 🧐
- Take home messages: be careful about: ⚠️ Indication creep (using a drug way beyond of studied patient populations). ⚠️ Dose adjustments that don’t make mathematical sense. ⚠️ Piling lots of coagulopathies on top of one another (eg uremic platelet dysfunction + aspirin + eptifibatide).

- Eventually he deteriorated to the point of requiring intubation. CT head showed a massive subdural hematoma. Teaching point #1: when new-onset delerium occurs always look for bad things. Subdural hematoma can exert diffuse pressure on the brain with minimal focal neuro findings.

- Review showed that the cause of the bleed was probably integrillin accumulation 2/2 renal failure. His GFR was <<30 All the RCTs on eptifibatide excluded patients with GFR <30! This is a classic example of indication creep: a drug is shown to be useful in a subset of patients ➡️ used too broadly

- "Heil Hitler" by Ye has been banned by nearly all digital streaming platforms. You can still watch it on twitter, though. Academic institutions, journals, et al. - is this *really* a platform that you want to be supporting and affiliating with?
- [Not loaded yet]
- got it stuck in my head and I think I need general anesthesia now
- fully grown adults with a longstanding history of being aweful don’t suddenly grow a better personality when put in a position of power. I hope you’re enjoying my sociology course, please be sure to give me a five-star review so I can get promoted.

- Pharmacokinetics of drug removal during plasma exchange (PLEX): You have a complex patient on several meds and you’re about to remove all the albumin in their body - how much does this affect medication levels? 🧵 #1/4 #EMIMCC

-
View full threadSo for the vast majority of drugs, all you need to do is make sure the drug is given well before PLEX or (ideally) right after PLEX. The time between drug administration and PLEX should be much longer than the distribution half-life so the drug has time to run into the tissues:

- Drugs with a very low Vd are in trouble because they can’t hide. The most common ones in this category are enoxaparin, heparin, and liposomal amphotericin. Heparin levels should rebound pretty fast but enoxaparin may require more dose adjustment. more at IBCC: emcrit.org/ibcc/pharmac... #4/4

- The key parameters are volume of distribution (Vd) and distribution half-life Most drugs have a Vd much higher than plasma volume (Vd >>0.05 L/kg) so they escape the plasma and arent removed much by PLEX BUT, to escape removal, the drug needs to distribute into the tissues before PLEX occurs. #2/4

- I'm updating the IBCC chapter on opioid use disorder. Any pearls/pitfalls or recent review articles? Would be especially interested to hear about methadone initiation & management of fentanyl-xylazine withdrawal 🙏

- [Not loaded yet]
- any thoughts on macro-induction (starting with 16 or 32 mg)? I think some of the studies on macro-induction were done at Yale.
- update: you have more clinical experience than the HHS secretary, NIH director, and surgeon general combined!
- ok, ok, ok, I understand the rationale for conducting a national talent search for the next department chair. but this really seems extra.
- doing LPs on therapeutic heparin or DOACs seems pretty insane to me. my main go-to source is the British Association of Neurologists guideline: pubmed.ncbi.nlm.nih.gov/30154234/ you can LP through DAPT if you really have to (IBCC discussion: emcrit.org/ibcc/id/#lum...)
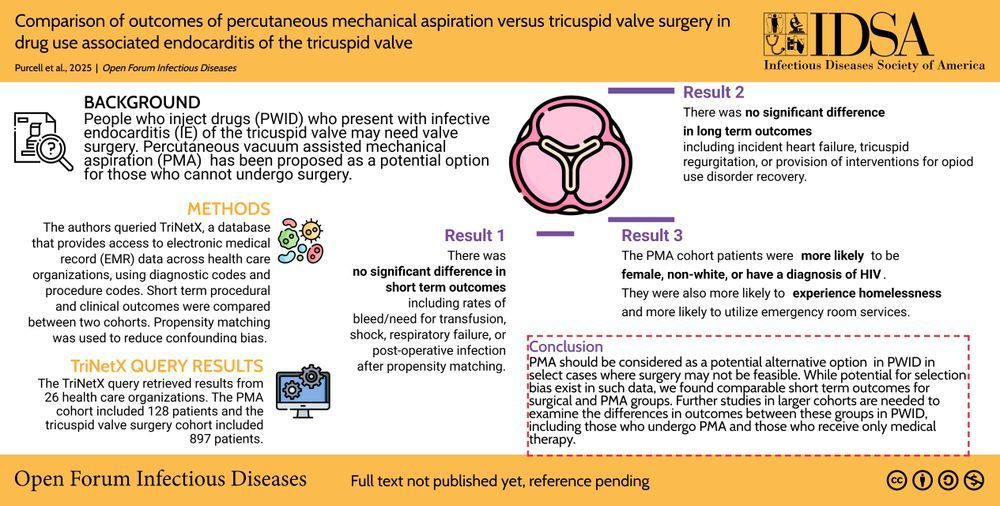
- I was skeptical about percutaneous mechanical aspiration for tricuspid valve endocarditis, but it apparently can work. Look at this picture of a vegetation that was fished out of a patient I was involved with. Only after removal was he able to achieve negative blood cultures.👇 #EMIMCC
- Comparison of outcomes of percutaneous mechanical aspiration versus tricuspid valve surgery in drug use associated endocarditis ✅ Just Accepted #IDSky
- [Not loaded yet]
- yeap, no combination of antibiotics will ever penetrate all the biofilms in that vegetation.
- [Not loaded yet]
- yeah, 2 thoughts: 1) tricuspid isn't super important, pts can do OK despite a moderately dysfunctional valve 2) even if you do need surgery eventually, its much better to cure the infection, rehab the pt, and do *elective* surgery (vs surgery when pt bacteremic and acutely ill w/ endocarditis)
- nocturnal alpha-2 agonists FTW 🥳 the MENDING RCT shows benefit from PO guanfacine 2 mg QHS in delirium (unpublished, data online here clinicaltrials.gov/study/NCT04742673?c…) logistically an oral medication seems more feasible #EMIMCC
- Any blood pressure data?
- according to the data up it looks like there was no difference in hypotension I wouldnt give guanfacine to a patient with hypotension or borderline BP but its really a pretty weak antihypertensive agent.
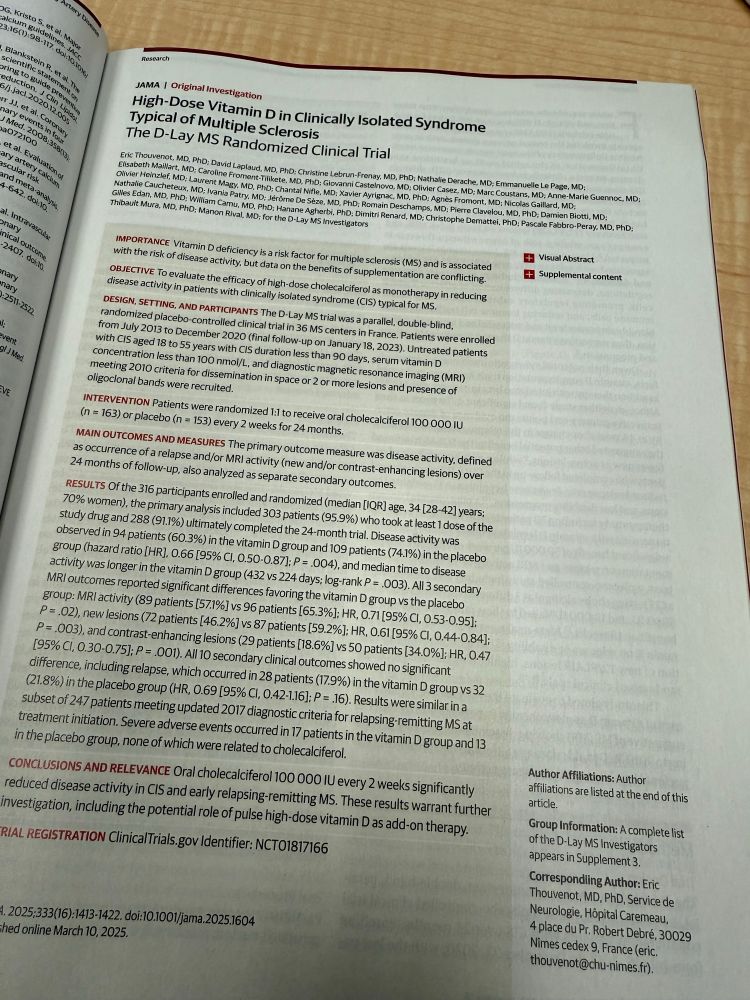
- He'll has frozen over! Pigs flew! Vitamin D worked in a placebo controlled RCT! Vitamin D reduced flares of clinically isolated syndrome typical of MS
- I would dare someone to try to replicate this. Based on the massive number of RCTs on vitamin D, eventually one will hit p-value gold purely by chance. Look how many hits this pubmed search got
- My face when I pop over there and still see old MedTwitter friends still posting

- adulting in 2025 is hard. I want to support medical education but not fascism. nobody warned me about this struggle in medical school.
- PO meds are so hot right now (PO=IV) but in critically ill patients (esp with enteral feeding tubes), the pharmacology gets tricky & data is often scant when the patient starts vomiting... do we redose everything? IMHO the default route for live-saving meds in ICU should still be IV #EMIMCC
- [Not loaded yet]
- I'm working on a section about drug dosing in plasma exchange and this is an interesting concept that I never really thought about.
- [Not loaded yet]
- [Not loaded yet]
- I struggle with this because greater reach does have real benefits in terms of education etc. But for now the fascism stuff is just a bridge too far for me.
- [Not loaded yet]
- I’m on a lot of social media platforms and the twitter for-me page is chok full of NSFW content - which is unlike any other platform After a while I think institutions are going to start questioning whether they really want to be associated with twitter. It’s not the same as it used to be.
- Everyone should ideally leave twitter and come to bluesky for several reasons. - Unify the discussion - Safe space for everyone (eg LGBTQ) - Stop supporting twitter (which is now a vehicle of misinformation & political manipulation) - Twitter is currently NSFW (eg frankly pornographic content)
- giving FFP to a patient with cirrhosis will make the INR look better but is unlikely to actually help the patient clot. INR reflects clinical coagulation for patients on warfarin, but not in cirrhosis/DIC. (emcrit.org/ibcc/cirrhosis/#coa…)
- [Not loaded yet]
- I agree with you 💯
- [Not loaded yet]
- every patient with cirrhosis needs 30 mg of iv phytonadione, if you give them a mg less than 30 then you’re a horrible irresponsible person (I still get this from some transplant centers)

- bucket list: write a one word note. “heparin” nothing more. I probably need to be more a more senior attending before I can get away with this.

- [Not loaded yet]
- I think you would REALLY need to be tenured to get away with that one