- I want to talk about a patient who died when I was a trainee. He presented with an MI & was treated w/ the usual therapies along with an eptifibatide infusion (an antiplatelet gtt which was commonly used back then). He developed agitated delirium refractory to numerous medications… #EMIMCC #1/5

- Eventually he deteriorated to the point of requiring intubation. CT head showed a massive subdural hematoma. Teaching point #1: when new-onset delerium occurs always look for bad things. Subdural hematoma can exert diffuse pressure on the brain with minimal focal neuro findings.

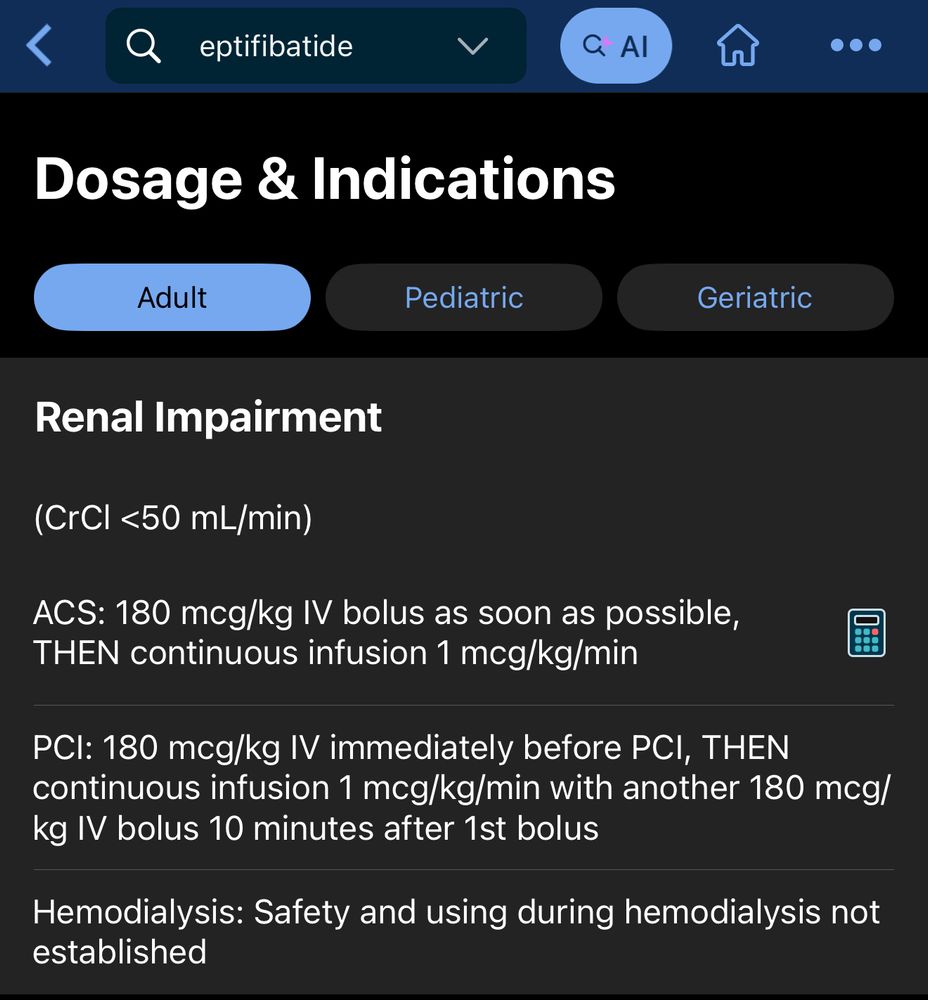
- Review showed that the cause of the bleed was probably integrillin accumulation 2/2 renal failure. His GFR was <<30 All the RCTs on eptifibatide excluded patients with GFR <30! This is a classic example of indication creep: a drug is shown to be useful in a subset of patients ➡️ used too broadly

- And to this day, the published dosing of eptifibatide doesn’t make much sense. You’re supposed to dose-reduce for GFR <50. But it doesn’t really make sense to give the same dose for GFR 49 & GFR 10 (the drug is renally cleared) 🧐
- Take home messages: be careful about: ⚠️ Indication creep (using a drug way beyond of studied patient populations). ⚠️ Dose adjustments that don’t make mathematical sense. ⚠️ Piling lots of coagulopathies on top of one another (eg uremic platelet dysfunction + aspirin + eptifibatide).May 10, 2025 21:42